
Healthcare and Heterogeneity: The Importance of Interculturality in Public Health
Interculturality and Public Health| Emily Mackie
I want you to take a moment to think about what it means to you to be healthy. Now think about your last trip to see a healthcare professional. Did you feel as though they listened to you and appreciated your perspective? Do you feel like you received care that aligned with your approach to health? Today’s globalised world is diverse and complex, and the unique context of each person’s being influences the way that they approach and receive healthcare. This was the key concept that was unpacked in the Intercultural Approaches to Public Health short course, which we were lucky enough to partake in at the Pontifical Catholic University of Chile in Santiago during the month of January this year. Set against the Chilean cultural and political backdrop, we explored what it means to take an intercultural approach to healthcare. In this article, we apply what we learned in this course to reflect on what it means to exercise interculturality in the context of the healthcare systems of our own respective countries: Aotearoa New Zealand, Australia, and Chile.
Emily – Aotearoa New Zealand
In Aotearoa New Zealand, interculturality in the context of health requires appreciation of the range of cultural values which intersect with healthcare in our country. To see how culture interacts with the healthcare landscape, it is important to understand our migratory history, including European colonisation. Today, Pākehā, or New Zealand Europeans, represent the largest ethnic group in the country, however prior to European colonisation in the 19th century, the land was inhabited solely by the Indigenous Māori people. In 1840, the Treaty of Waitangi was signed, which provided a legally binding partnership agreement between Māori Iwi and the Crown, promising Crown protection of Māori and Māori autonomy over their resources [1]. Over the following century, there was an influx of immigrants from Britain in search of a better life [2]. In the second half of the 20th century, greater numbers of migrants from other parts of the world, such as Asia and the Pacific, began to arrive [3]. Today, Aotearoa New Zealand is an increasingly culturally diverse country, home to people from over 200 different birthplaces [4]. This diversity brings with it a range of different experiences, perspectives, and attitudes, which influence the way that different people go about life, including how they interact with and are served by healthcare.
In Aotearoa New Zealand, publicly funded healthcare is available to all residents [5]. Alternatively, those who can afford it can pay for private healthcare, which generally offers shorter wait times for treatments. This healthcare system is scaffolded by a legislative framework [1], which includes laws such as the Health Act of 1956. Despite this public health system, healthcare is not experienced equally across all groups in the country. For example, in comparison to Pākeha, Māori are disproportionately affected by chronic disease and are more likely to suffer from mental health conditions [6]. Other groups also face poorer health outcomes than Pākehā. For example, Pasifika New Zealanders have a life expectancy that is on average six years shorter [7]. These disparities are produced by complex socioeconomic factors, deeply rooted in the effects of colonisation that persist in Aotearoa New Zealand’s institutions today [8]. The concept of equity was not even considered in government health policy until 1993 [9].
Recently, measures have been taken to move towards more equitable health outcomes for all groups in Aotearoa New Zealand, including Māori. An independent investigation found that the government had failed to actively address Māori health inequity, and that this was a breach of the Treaty of Waitangi [10]. This led to the installation of the Pae Ora (Healthy Futures) Act in 2022, a piece of health legislation with the purpose of promoting health for all New Zealanders and reducing health inequities across different groups [1]. Having this legislation in place is essential for moving towards a future where all Kiwis are guaranteed the same quality of healthcare, however it is important that this is complemented by intercultural approaches at all levels of health. This includes moving away from a single, Western epistemology regarding medicine and well-being, and adapting the system to value other worldviews not as secondary to Western medicine, but as equally valid; one example is centering models such as Te Whare Tapa Whā, the model of Māori health developed by Tā Mason Durie in 1984 [11]. This highlights the critical nature of factors such as wairua (spiritual) and whanau (family) health for overall well-being, an idea which is not common in European models of health.
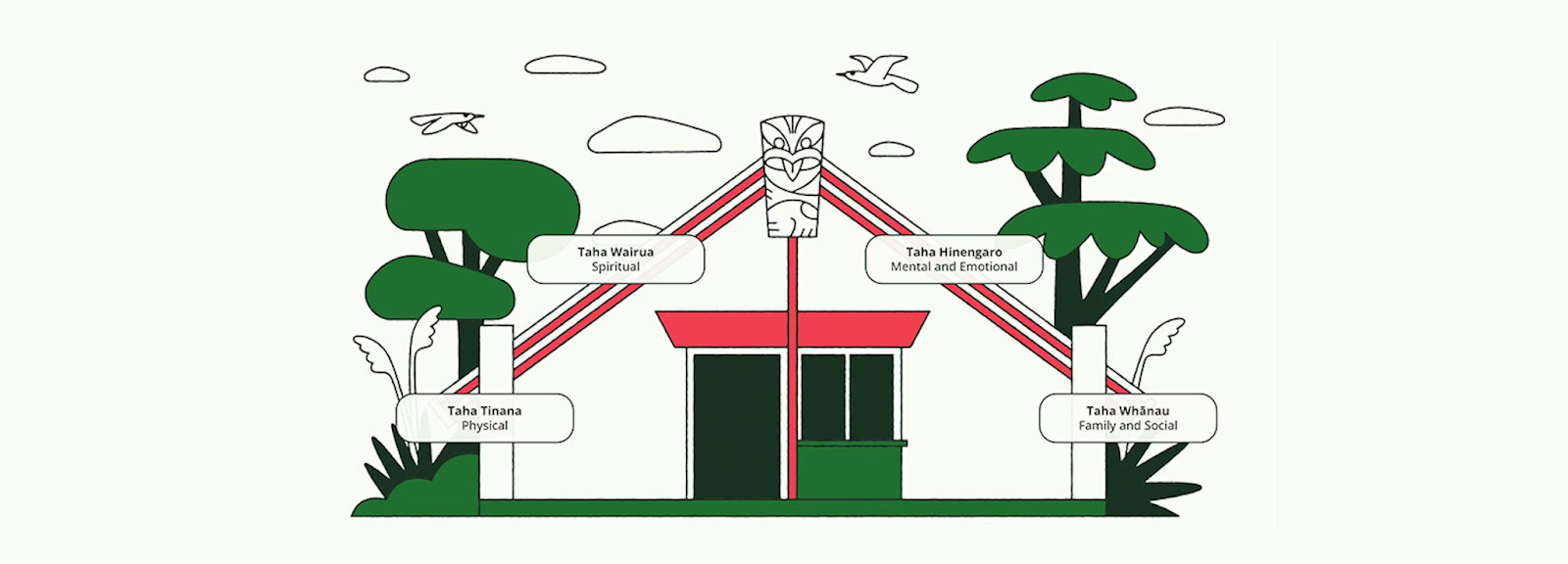
Figure 1: A whare (meeting house) depicting the Te Whare Tapa Whā model of Māori health. This emphasises the collective importance of Tinana, Wairua, Hinengaro, and Whānau in creating well-being. Image from the New Zealand Institute of Skills and Technology [12].

Figure 2: Aboriginal women prepare bush medicine at the Akeyulerre healing centre in Alice Springs, Australia. Image from ABC News [17].
But multiculturalism is not interculturalism, and while multicultural societies have their benefits, they also have distinct limitations as they flatten and dissolve the distinctions between communities. Instead, an intercultural approach to public health results in diverse and pluralistic communities being acknowledged, and their needs met.
In recent years, the Australian healthcare system has seen a marked transformation in its approach to interculturality in healthcare, with a particular focus on services for First Nations and culturally and linguistically diverse (CALD) communities. These services are underpinned by several key tenets, namely that they are place-based, locally led, and prioritise delivery by people with lived experience [20]. This presents a departure from the conventional Western paradigm that supports a one-size-fits-all approach to healthcare [21]. While this approach indicates significant investment on the part of the Australian public health system, in thought, commitment, and resources it is by no means the end of the road.
For Australia to truly adopt a meaningful intercultural approach to public health, it would require further integration of traditional knowledge systems as equal to the biomedical Western models, not just complementary. As integrated healthcare services continue to be developed and prioritised in conjunction with the synthesis of culturally-safe research and praxis, interculturality can be embedded as the default public health paradigm in Australia.
Mariela – Australia
Healthcare in Australia is over 60,000 years old, with the longest living cultures in the world residing across the continent [13]. The cosmologies of the hundreds of First Nations that have lived in Australia since time immemorial reflect the profound interconnectedness between communities and Country [14]. Part of this connection to Country involves components that concern the spiritual and social determinants of health, complemented by the support of physical health through bush medicine practices [15]. However, since British colonisation in 1788, Australia’s dominant healthcare system has adopted the Western biomedical model [14]. This has resulted in significant impacts to First Nations health, with Indigenous communities experiencing significant disparities in life expectancy and rates of chronic disease compared to their non-Indigenous counterparts [16]. This Western model of healthcare as it plays out in Australia is particularly damaging due to its insistence on the separation of mind and body, and the dismissal of additional components of health such as connection to land and community [16].
In the 237 years since colonisation, Australia has experienced waves of immigration that have influenced the highly multicultural society the country prides itself on today. These cultures have brought their own healthcare systems and practices that have been loosely integrated into the healthcare system, such as Chinese traditional medicine and Ayurvedic clinics [18]. Marking a significant milestone in the movement towards a more inclusive and integrated public healthcare system, the Australian Federal Government announced the creation of a new Multicultural Health Consumer and Carer Network in 2024 [19]. This exists in addition to alternative primary health care networks, such as the Aboriginal Community Controlled Health Organisations, that complement the mainstream public health system.
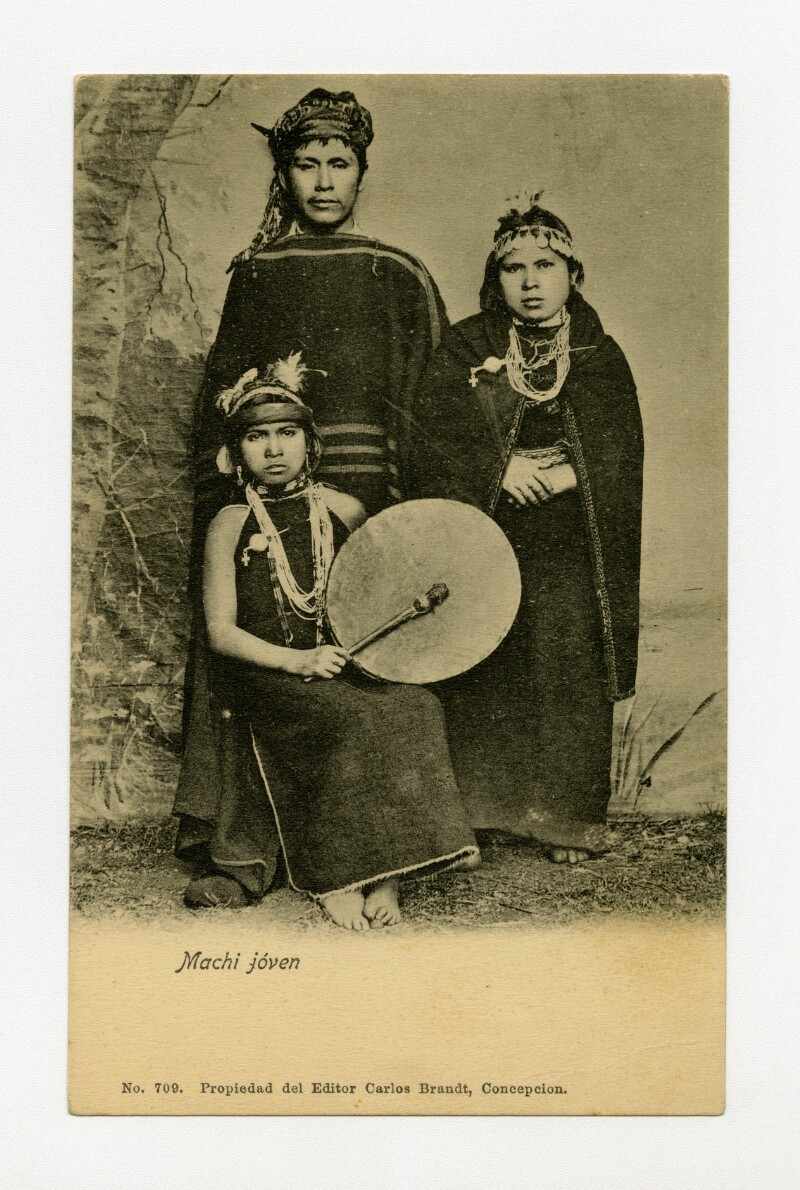
Figure 3: A postcard from the late 19th century depicting a young Mapuche Machi. In Mapuche culture, a Machi is a spiritually assigned healer who treats illness by restoring their patient’s balance with nature in healing ceremonies [29]. Image from La Biblioteca Nacional de Chile [30].
However, the cultural landscape is shifting, and the system now must accommodate a multicultural society influenced by migration from countries like Haiti, Venezuela, and Colombia. This introduces new challenges, such as the need for Creole translators and a deeper understanding of different cultural perceptions regarding maternal health and nutrition [31]. True interculturality requires healthcare providers to move beyond simple “tolerance” and toward an active integration of these varying perspectives on the human body. To improve the current state of public health, Chile must move beyond token inclusion. While having a traditional healer in a hospital is a start, the core medical and health sciences curricula in universities still largely ignore non-Western epistemologies [32]. Improvements should focus on formalizing intercultural competence as a mandatory skill for all health professionals, not just those working in rural areas [33]. Additionally, there is a need for better infrastructure that reflects local architecture and rituals. By evolving the system to treat the person within their specific cultural context, Chile can move toward a more equitable and truly “public” health model that heals the social fabric alongside the physical body.

Nicole – Chile
An intercultural approach to public health in Chile represents a fundamental shift from a rigid, monolithic biomedical model toward one that recognises the diverse cosmovisions of its inhabitants. In the Chilean context, this primarily involves the intersection between the modern state healthcare system and the ancestral knowledge of Indigenous peoples—such as the Mapuche, Aymara, and Rapa Nui—as well as the rapidly growing migrant populations from across Latin America and the Caribbean [22]. For a country that has historically functioned under a centralised and standardised medical authority, moving towards interculturality means acknowledging that “health” is not merely the absence of biological pathology, but a state of equilibrium between the individual, the community, and the natural environment [23]. Currently, the Chilean healthcare system is structured around a dual model: the public National Health Fund (FONASA) and the private health insurance institutions (ISAPRE) [24]. The vast majority of the population, including nearly all Indigenous and migrant groups, relies on the public system for their medical needs. Within this framework, the government has implemented the Program for Health and Indigenous Peoples (PESPI). This program is a significant step towards accommodation, as it seeks to reduce cultural barriers and incorporate traditional healing practices alongside Western medicine [25], [26]. In regions with high Indigenous populations, such as Araucanía, it is now possible to find intercultural hospital modules where a Machi (Mapuche healer) works in coordination with medical doctors [27]. These spaces allow for traditional ceremonies and the use of herbal medicine, providing cultural safety for patients who might otherwise feel alienated by cold, clinical environments [28].
The concept of interculturality involves not just the recognition of the diversity that exists in a society, but rather the dynamic appreciation of cultural difference. The health and well-being of an individual are determined by the network of factors which shape that individual’s life, including (but not limited to) education, nutrition, environment, social norms, and economic and political systems [35]. These conditions create individual context, which in turn influences the way that each person views the world, and health by extension. Health inequity is perpetuated when healthcare systems fail to appreciate and accommodate cultural heterogeneity. This is apparent in Aotearoa New Zealand, Australia, and Chile, where intercultural approaches are needed to address gaps in health outcomes, particularly between Indigenous and non-Indigenous people. Every person deserves to experience good health, however that may look to them. It is by creating dialogue, mutual respect, understanding, and empowering communities to advocate for their health that this can be achieved.
[1] Ministry of Health New Zealand, “Health system overview and statutory framework.” Accessed: Mar. 18, 2026. [Online]. Available: https://www.health.govt.nz/about-us/new-zealands-health-system/overview-and-statutory-framework.
[2] J. Phillips, “British immigration and the New Zealand Company,” Te Ara – the Encyclopedia of New Zealand. Accessed: Mar. 20, 2026. [Online]. Available: https://teara.govt.nz/en/history-of-immigration/page-3
[3] J. Phillips, “The end of a ‘white New Zealand’ policy,” Te Ara – the Encyclopedia of New Zealand. Accessed: Mar. 20, 2026. [Online]. Available: https://teara.govt.nz/en/history-of-immigration/page-15.
[4] Stats NZ, “Census results reflect Aotearoa New Zealand’s diversity.” Accessed: Mar. 18, 2026. [Online]. Available: https://www.stats.govt.nz/news/census-results-reflect-aotearoa-new-zealands-diversity/.
[5] Immigration New Zealand, “Who can get public health care.” Accessed: Mar. 18, 2026. [Online]. Available: https://www.immigration.govt.nz/live/setting-up-your-life-in-new-zealand/getting-health-care-and-finding-a-doctor/who-can-get-public-health-care/
[6] J. Gurney and J. Koea, “Breaking the inequity loop,” Public Health Expert Briefing. Accessed: Mar. 20, 2026. [Online]. Available: https://www.phcc.org.nz/briefing/breaking-inequity-loop.
[7] Health New Zealand – Te Whatu Ora, “Health Status Report 2023,” Wellington, New Zealand, Feb. 2024. [Online]. Available: https://www.tewhatuora.govt.nz/assets/Publications/Health-status-reports/HNZ-TWO-Health-Status-Report_FULL.pdf.
[8] M. Hobbs, A. Ahuriri-Driscoll, L. Marek, M. Campbell, M. Tomintz, and S. Kingham, “Reducing health inequity for Māori people in New Zealand,” Lancet, vol. 394, no. 10209, pp. 1613–1614, Nov. 2019, doi: https://doi.org/10.1016/s0140-6736(19)30044-3.
[9] Ministry of Health New Zealand, “Achieving Equity in Health Outcomes: Highlights of Important National and International Papers,” Wellington, New Zealand, Sep. 2018. [Online]. Available: https://www.health.govt.nz/system/files/2018-11/achieving-equity-in-health-outcomes-important-paper-highlights-nov18_1.pdf.
[10] N. Sheridan et al., “Hauora Māori – Māori health: a right to equal outcomes in primary care,” Int. J. Equity Health, vol. 23, Feb. 2024, doi: https://doi.org/10.1186/s12939-023-02071-6.
[11] Mental Health Foundation, “Te Whare Tapa Whā.” Accessed: Mar. 22, 2026. [Online]. Available: https://mentalhealth.org.nz/te-whare-tapa-wha.
[12] New Zealand Institute of Skills and Technology, “Te Whare Tapa Whā.” Accessed: Mar. 22, 2026. [Online]. Available: https://www.nzist.ac.nz/te-pae-ora/living-well-learning-well/te-whare-tapa-wha.
[13] P. Saunders, A. Barnes, R. Dashwood, and K. Doyle, “Learning across the life course: A trans-education approach to develop Indigenous intercultural potential in healthcare,” First Nations Health and Wellbeing – The Lowitja Journal, vol. 2, p. 100032, Oct. 2024, doi: 10.1016/j.fnhli.2024.100032.
[14] G. D. Asamoah, M. Khakpour, T. Carr, and G. Groot, “Exploring Indigenous Traditional Healing programs in Canada, Australia, and New Zealand: A scoping review,” Explore, vol. 19, no. 1, pp. 14–25, Jan.–Feb. 2023, doi: 10.1016/j.explore.2022.06.004.
[15] A. Gall, K. Anderson, J. Adams, V. Matthews, and G. Garvey, “An exploration of healthcare providers’ experiences and perspectives of Traditional and complementary medicine usage and disclosure by Indigenous cancer patients,” Complementary Altern. Med., vol. 19, Sept. 2019, doi: 10.1186/s12906-019-2665-7.
[16] K. Ngampromwonse and A. Gall, “10 years of preventive health in Australia. Part 2 – centring First Nations sovereignty,” Public Health Res. Pract., vol. 35, no. 2, p. PU24023, May 2025, doi: 10.1071/PU24023.
[17] E. Haskin, “‘Bush medicine heals ailments but also keeps Indigenous women's culture alive and well,” ABC. Accessed: Mar. 24, 2026. [Online]. Available: https://www.abc.net.au/news/2019-09-28/bush-medicine-keeping-womens-culture-alive-and-well/11545810.
[18] J. Agu, “Traditional medicines must be integrated into health care for culturally diverse groups,” The Conversation. Accessed: Mar. 21, 2026. [Online]. Available: https://theconversation.com/traditional-medicines-must-be-integrated-into-health-care-for-culturally-diverse-groups-114980.
[19] Department of Health, Disability and Ageing Australia, “Giving CALD Australians a say: new Health Consumer and Carer Network,” Sept. 3, 2024. [Online]. Available: https://www.health.gov.au/ministers/the-hon-ged-kearney-mp/media/giving-cald-australians-a-say-new-health-consumer-and-carer-network.
[20] A. Clifford-Motopi, J. Stajic, J. Ward, and A. Shakeshaft, “‘We are experts in telling our story’: the perspectives of stakeholders from Aboriginal Community-Controlled Health Services on the health and wellbeing of urban First Nations Australians, and their priorities for a First Nations urban health research agenda in Australia,” Prim. Health Care Res. Dev., vol. 27, pp. 1–7, Nov., 2025, doi: 0.1017/S1463423625100807.
[21] K. Clapham et al., “Shifting sands: Indigenous conceptions of health and place in fragile times,” Health & Place, vol. 89, Sept., 2024, doi: 10.1016/j.healthplace.2024.103308.
[22] M. Poblete and E. Goldstein, “Políticas de Salud Intercultural en Chile,” Biblioteca del Congreso Nacional de Chile, Valparaíso, Chile, July 2019. [Online]. Available: https://obtienearchivo.bcn.cl/obtienearchivo?id=repositorio/10221/27514/1/BCN_Poblete___Politicas_de_Salud_Intercultural_en_Chile_final.pdf.
[23] P. González, “Salud intercultural y normativas,” Revista del Colegio Médico de Chile, Aug. 4, 2023. [Online]. Available: https://revista.colegiomedico.cl/salud-intercultural-y-normativas/.
[24] Superintendencia de Salud, “Cómo funciona el sistema de salud en Chile.” [Online]. Available: https://www.superdesalud.gob.cl/orientacion-en-salud/como-funciona-el-sistema-de-salud-en-chile/.
[25] Servicio de Salud Metropolitano Sur, "Programa Especial de Salud y Pueblos Indígenas (PESPI)." [Online]. Available: https://ssms.gob.cl/como-me-cuido/programas-de-salud/programa-especial-de-salud-y-pueblos-indigenas-pespi/.
[26] Servicio de Salud Metropolitano Sur Oriente, "Programa Especial de Salud y Pueblos Indígenas (PESPI)." [Online]. Available: https://redsalud.ssmso.cl/programa-especial-de-salud-y-pueblos-indigenas-pespi/.
[27] Ministerio de Salud de Chile, “Orientaciones para la Planificación y Programación en Red,” Res. Exenta Nº 196, Sept. 2024. [Online]. Available: https://www.minsal.cl/wp-content/uploads/2024/09/RES.-EXENTA-N%C2%B0-196-ORIENTACIONES-PARA-LA-PLANIFICACION-Y-PROGRAMACION-EN-RED-.pdf.
[28] Biblioteca del Congreso Nacional de Chile, "Ley 20584: Regula los derechos y deberes que tienen las personas en relación con acciones vinculadas a su atención en salud," Apr. 2012. [Online]. Available: https://www.bcn.cl/leychile/navegar?idNorma=1039348.
[29] Museo Chileno de Arte Precolombino, “Machi Kimün. Yesterday and today.” Accessed: Mar. 24, 2026. [Online]. Available: https://museo.precolombino.cl/chamanismo/en/11-machi-kimun-yesterday-and-today/.
[30] C. Brandt, “Machi jóven,” Archivo Fotográfico de Biblioteca Nacional Digital de Chile. [Photo]. Available: https://www.bibliotecanacionaldigital.gob.cl/bnd/629/w3-article-614078.html
[31] M. N. Manríquez-Hizaut, C. Lagos-Fernández, J. Rebolledo-Sanhuesa, and V. Figueroa-Huencho, "Salud intercultural en Chile: Desarrollo histórico y desafíos actuales," Revista de Salud Pública, vol. 20, no. 6, pp. 759-763, 2018, doi: 10.15446/rsap.v20n6.65625.
[32] Ministerio de Salud de Chile, "Decreto 17: Aprueba reglamento sobre el derecho de las personas pertenecientes a pueblos indígenas a recibir atención de salud con pertinencia cultural," July 2023. [Online]. Available: https://www.bcn.cl/leychile/navegar?idNorma=1199560.
[33] Subsecretaría de Previsión Social, "Sistema de Salud." [Online]. Available: https://previsionsocial.gob.cl/organizaciones/organizaciones-gremiales-y-sindicales/sistema-de-salud/.
[34] Z. S. Rice and P. Liamputtong, “Culture and Global Health,” Handbook of Global Health, pp. 1–26, July 2020, doi: 10.1007/978-3-030-05325-3_56-1.
[35] WHO, “Social determinants of health.” Accessed: Mar. 23, 2026. [Online]. Available: https://www.who.int/news-room/fact-sheets/detail/social-determinants-of-health.

Emily is currently completing a Masters of Biomedical Science, focusing on molecular genetics in the context of human health. Outside the lab, her role as the co-vice president of the Scientific keeps her busy. She also enjoys hiking, photography, painting, and writing.